CMS has released new implementation details for Calendar Year 2027 risk adjustment, and the operational message is clear: Medicare Advantage organizations need to prepare now for a more encounter-linked, documentation-driven risk adjustment environment.
The July 9, 2026 HPMS memo confirms several important implementation details, including continued use of the 2024 CMS-HCC model for CY 2027, the use of the 2027 RxHCC model, updated normalization factors, changes to diagnosis sources, MAO-004 reporting updates, and the timing of when key exclusions will affect risk scores and payments.
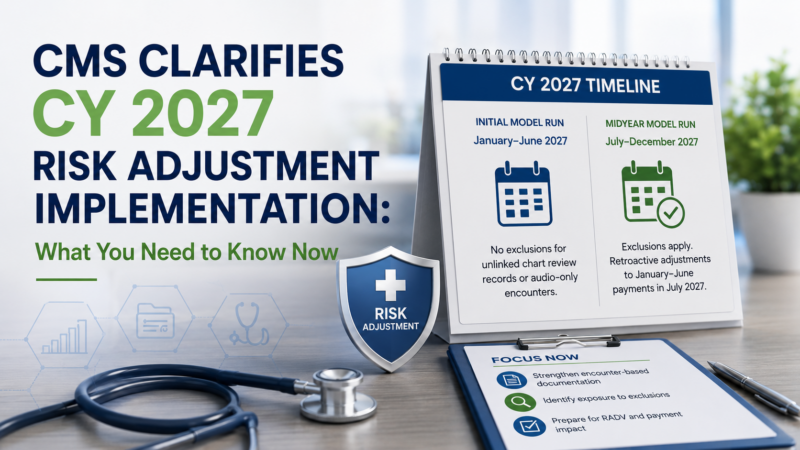
Most importantly, CMS confirmed that diagnoses from unlinked chart review records and certain audio-only encounters will be excluded from risk score calculation beginning with the CY 2027 Midyear model run.
That timing matters. While the exclusions will not affect the CY 2027 Initial model run, they will affect Midyear risk scores, payments for July through December, and retroactive adjustments to payments for January through June.
For Medicare Advantage plans, this creates a limited operational window to identify exposure, strengthen encounter-based workflows, and ensure diagnosis capture is supported before the new exclusions are reflected in payment.
CMS released implementation information for CY 2027 risk adjustment models, normalization factors, diagnosis source exclusions, MAO-004 reporting updates, Model Output Reports, and risk adjustment model software.
For organizations other than PACE, CMS will continue using the 2024 CMS-HCC model to calculate risk scores in CY 2027. CMS will also continue using the 2023 ESRD model for beneficiaries in dialysis, transplant, and post-graft status.
For Part D, CMS will use the 2027 RxHCC model calibrated to 2023 and 2024 data, with separate continuing-enrollee model segments for MA-PD plans and stand-alone PDPs.
For PACE organizations, CMS will continue a blended methodology across CMS-HCC, ESRD, and RxHCC models, using a 50 percent blend of newer encounter data and FFS-based models with older models that include RAPS, encounter data, and FFS claims.
For most Medicare Advantage organizations, however, the most operationally important section of the memo is not the model list. It is the section on sources of diagnoses.
CMS finalized changes to the diagnoses that can be used for the CY 2027 risk score calculation. Two exclusions are especially important:
CMS will delay implementation of these exclusions until the CY 2027 Midyear risk adjustment model run.
That means the CY 2027 Initial model run will not exclude diagnoses from unlinked chart review records or affected audio-only encounters. But the CY 2027 Midyear model run will.
This creates an important timing issue for plans. Payments from January through June 2027 will initially be based on risk scores that do not reflect the exclusions. But payments from July through December 2027 will reflect the exclusions, and CMS will make retroactive adjustments to payments from January through June in July 2027 if Midyear risk scores differ from Initial risk scores.
In other words: plans may not feel the impact immediately in January 2027, but that does not mean the impact is not coming.
For non-PACE organizations, CMS confirmed that diagnoses from unlinked chart review records with 2026 dates of service will be excluded from risk score calculation beginning with the CY 2027 Midyear model run.
An unlinked chart review record is a chart review diagnosis that is not tied to a specific encounter. This matters because risk adjustment is moving toward a more encounter-based standard. Diagnoses need to be supported by documented clinical evidence connected to an eligible encounter.
CMS will allow an exception for beneficiaries who switch from one Medicare Advantage contract to another contract in a different parent organization. In those cases, diagnoses from unlinked chart review records may still be considered if CMS verifies that the parent organization effective on the date of service differs from the parent organization effective at the time of submission.
For most plans, however, the direction is clear: unlinked retrospective diagnosis capture is becoming less reliable as a risk adjustment strategy.
CMS also finalized that diagnoses from audio-only services identified using the modifiers “93” or “FQ” will be excluded from risk score calculations beginning with the CY 2027 Midyear model run.
The exclusion applies to diagnoses from professional and outpatient encounter data, chart review records, and FFS claims with 2026 dates of service, when all risk-adjustment-eligible CPT/HCPCS line items associated with the record or claim have modifier “93” or “FQ.”
CMS clarified that if one or more risk-adjustment-eligible service lines do not have modifier “93” or “FQ,” all header diagnoses will be included for risk score consideration.
The operational takeaway is that plans and providers need to be precise with modifier use, telehealth workflows, and provider education. Diagnosis capture needs to reflect CMS’s face-to-face encounter requirements, and organizations should ensure that coding and documentation teams understand how audio-only services will be treated in CY 2027 payment.
The CY 2027 Midyear model run is where the implementation becomes financially meaningful.
CMS explained that:
Because the exclusions begin with the Midyear run, plans should not interpret the Initial run as a clean indicator of their CY 2027 exposure.
The more important question is: what happens when CMS reprocesses risk scores with unlinked chart review and audio-only exclusions applied?
That is where plans may see risk scores shift. That is also where January through June 2027 payments may be adjusted retroactively.
CMS is updating the MAO-004 report to address the CY 2027 diagnosis exclusions.
For January through September 2026 submissions, CMS will issue two sets of MAO-004 reports:
Beginning with the November report for October 2026 submissions, MAO-004 reports will exclude unlinked chart review diagnoses and audio-only encounters with modifier 93 or FQ.
CMS will also add a new Allow/Disallow Reason Code “U” for diagnoses disallowed because of the unlinked chart review exclusion when the parent organization switcher exception does not apply. The audio-only exclusion will be included under the current Allow/Disallow Reason Code “H.”
For risk adjustment teams, this makes MAO-004 monitoring even more important. Plans should be prepared to compare report sets, identify which diagnoses are being excluded, and understand how those exclusions affect payment and risk score projections.
CMS stated that there will be no new Model Output Report record types for CY 2027.
For organizations other than PACE, the relevant MOR record types include:
PACE organizations will also continue to receive MOR record types tied to blended model calculations, including record types K, B, and 7 for RAPS, encounter data, and FFS-based models.
While the MOR record types are not changing, plans still need to understand how the underlying exclusions affect which HCCs and RxHCCs appear in output files. The operational challenge is not simply reading the report. It is tracing which diagnoses were accepted, which were excluded, and why.
CMS also confirmed that it is continuing the transition of risk adjustment model software from SAS to Python.
For the CY 2027 Initial software, CMS has made both SAS and Python software available. CMS expects to provide both SAS and Python software for the CY 2027 Midyear/Final software later in 2026.
Beginning with CY 2028 Initial software, CMS intends to release risk adjustment model software only in Python.
This is not the headline risk adjustment change for most plans, but it is operationally important. Analytics, actuarial, and data teams that still rely heavily on SAS-based workflows should begin planning for the transition to Python now.
The CMS memo provides plans with more implementation details and also creates a clear action plan.
Plans should identify what percentage of risk-eligible diagnoses currently come from unlinked chart review records.
This is the starting point. Organizations cannot model the financial impact of the exclusion without understanding how much of their current risk adjustment performance depends on diagnoses that may no longer count.
Key questions to ask:
The exclusion of unlinked chart review records reinforces the need for prospective and encounter-linked documentation.
Organizations should prioritize workflows that bring HCC identification, validation, and documentation closer to the patient encounter.
That includes:
The goal is not simply to replace retrospective chart review with more manual work. The goal is to build a connected workflow where diagnoses are surfaced, validated, documented, and submitted in a way that ties back to the encounter.
Because diagnoses from audio-only services with modifier 93 or FQ will be excluded under specific conditions, plans should review how these modifiers are used across provider groups and encounter submissions.
Plans should evaluate:
This should be treated as both a coding education issue and an encounter data integrity issue.
The November 2026 reissued MAO-004 reports will be a critical operational checkpoint.
Plans should be ready to compare the initial and reissued report sets to determine:
Teams should also prepare to interpret the new “U” disallow reason code and existing “H” reason code in the context of CY 2027 risk score calculations.
The Initial model run may not show the full impact of the finalized exclusions. Plans should model potential changes before the Midyear run, not after.
That modeling should include:
The plans best prepared for CY 2027 will be those that anticipate the Midyear cliff before it arrives.
Although the memo is directed to Medicare Advantage organizations, Prescription Drug Plans, Cost Plans, and PACE organizations, provider organizations should still pay close attention.
Why? Because the operational burden of risk adjustment documentation sits heavily inside the clinical workflow.
If plans need more encounter-linked diagnosis support, providers will be expected to document more clearly, more specifically, and closer to the point of care.
That makes provider workflow design critical.
Health systems and provider groups should expect more emphasis on:
For providers, the question is not only whether diagnoses are captured. It is whether diagnoses are captured in a way that is current, specific, supported, and linked to the clinical encounter.
CMS’s CY 2027 implementation memo does not change the direction of risk adjustment policy. It clarifies how quickly organizations need to operationalize it.
Unlinked chart review diagnoses and certain audio-only diagnoses may not affect the Initial CY 2027 model run, but they will affect the Midyear model run. That means organizations have a short window to understand exposure, adjust workflows, and prepare for payment impacts.
The direction is clear: risk adjustment performance needs to be built into the encounter, not reconstructed after it.
Medicare Advantage organizations that continue to rely heavily on unlinked retrospective diagnosis capture may face greater revenue risk, reporting complexity, and audit exposure.
Organizations that build encounter-based workflows now will be better positioned for CY 2027 and beyond.
The main operational change is that CMS will exclude diagnoses from unlinked chart review records for non-PACE organizations and diagnoses from certain audio-only services with modifier 93 or FQ beginning with the CY 2027 Midyear model run.
No. CMS stated that diagnoses from unlinked chart review records will not be excluded during the CY 2027 Initial model run. The exclusion begins with the CY 2027 Midyear model run.
The exclusion will affect payments made for July through December 2027, which are based on the CY 2027 Midyear model run. If Midyear risk scores differ from Initial risk scores, CMS will also make retroactive adjustments to January through June 2027 payments in July 2027.
Beginning with the CY 2027 Midyear model run, CMS will exclude diagnoses from audio-only encounter records or claims with modifier 93 or FQ when all risk adjustment eligible CPT/HCPCS line items associated with the record or claim have one of those modifiers.
No. CMS stated that this change applies to CY 2027, using 2026 dates of service. It does not change filtering logic or submission guidance for prior years.
CMS will allow diagnoses from unlinked chart review records to be considered when a beneficiary switches from a Medicare Advantage contract in one parent organization to a contract in a different parent organization. CMS will verify the parent organization effective on the date of service against the parent organization effective at the time of submission.
CMS will reissue MAO-004 reports in November 2026 for January through September 2026 submissions. These reissued reports will exclude unlinked chart-review diagnoses and affected audio-only diagnoses. CMS will also add Allow/Disallow Reason Code “U” for unlinked chart review exclusions.
No. CMS stated that there are no new MOR record types for CY 2027.
For organizations other than PACE, CMS will continue to use the 2024 CMS-HCC model for CY 2027 risk scores. CMS will also use the 2023 ESRD model and the 2027 RxHCC model calibrated on 2023 and 2024 data.
MA plans should quantify unlinked chart review exposure, review audio-only encounter workflows, prepare for MAO-004 reporting changes, model Midyear payment impact, and move more HCC documentation into encounter-based workflows before the CY 2027 Midyear model run.
Need to understand where your CY 2027 risk adjustment workflow is exposed?
Inferscience helps healthcare organizations strengthen encounter-based HCC documentation, improve coding accuracy, and prepare for changing CMS requirements inside the clinical workflow.
Contact Inferscience to learn how to get your risk adjustment strategy 2027-ready.